In the age of electronic amusement, online port video games have become one of the most preferred kinds of gambling. These virtual devices are made to duplicate the excitement of playing букмекерська контора фавбет in an actual casino site, using players the opportunity to win big from the comfort of their own (more…)
Blog
-
Endometriosis Isn’t Just Painful Periods—Here’s What It Really Is
Across Africa, many women are told their severe period pain is “normal” or “that is just part of being a woman.” But for those living with endometriosis, the pain goes far beyond cramps.
The chronic pelvic pain associated with endometriosis can affect your education, career, intimacy, fertility, and emotional wellbeing, long before a diagnosis is made.
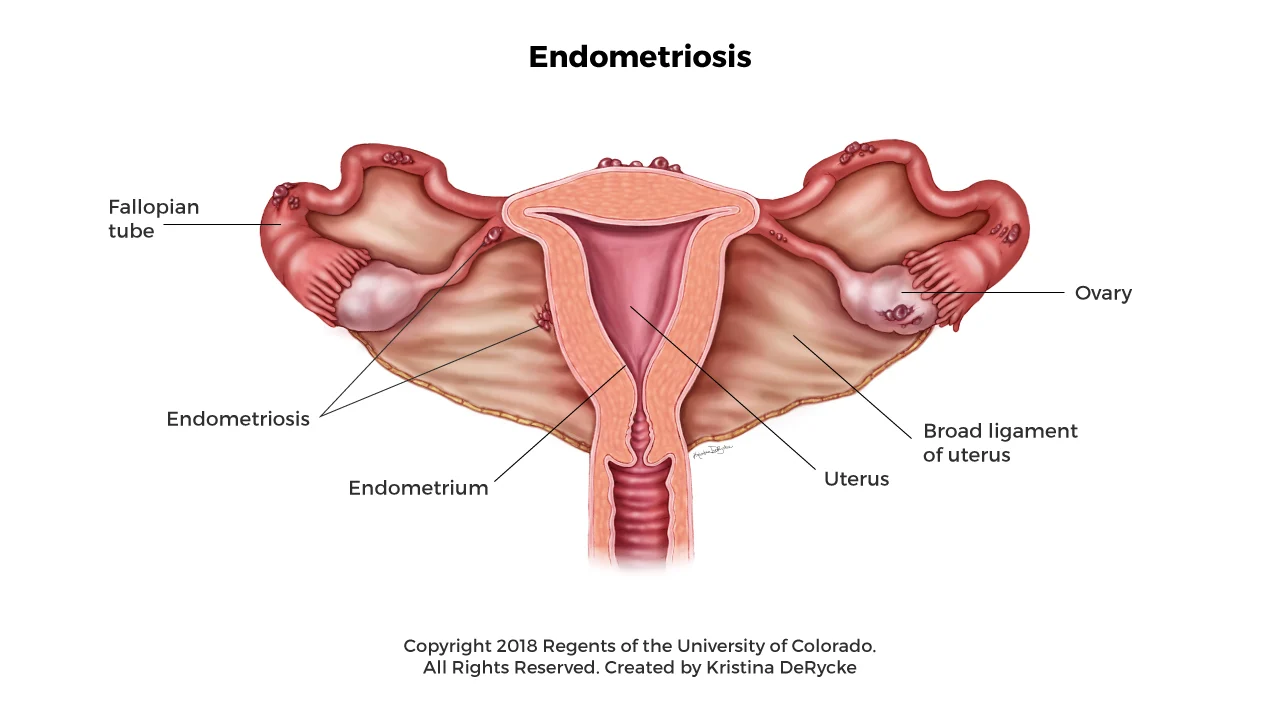
What Is Endometriosis?
Endometriosis is a condition where tissue similar to the lining of the womb grows in places it shouldn’t. Instead of staying inside the uterus, it can grow on the:
- ovaries
- fallopian tubes
- outer wall of the uterus
- pelvic lining
- bowel
- bladder
- diaphragm or chest (in rare cases)
This tissue responds to your menstrual cycle hormones, mainly estrogen and progesterone in the same way the uterine lining does.
During each cycle, it thickens, breaks down, and bleeds, but because it’s outside the womb, the blood has nowhere to go.
Over time, this trapped bleeding leads to:
- swelling and inflammation
- scar tissue
- organs sticking together (adhesions)
- chronic pelvic and back pain
Some people have intense symptoms. Others have mild or no pain at all but still experience complications like infertility.
Endometriosis often begins in the teenage years or early adulthood, but many people aren’t diagnosed until their 30s or 40s.
What Causes Endometriosis?
The exact cause of endometriosis isn’t fully understood, but experts believe several factors may play a role. For some people, genetics are involved, which is why the condition can appear across generations.
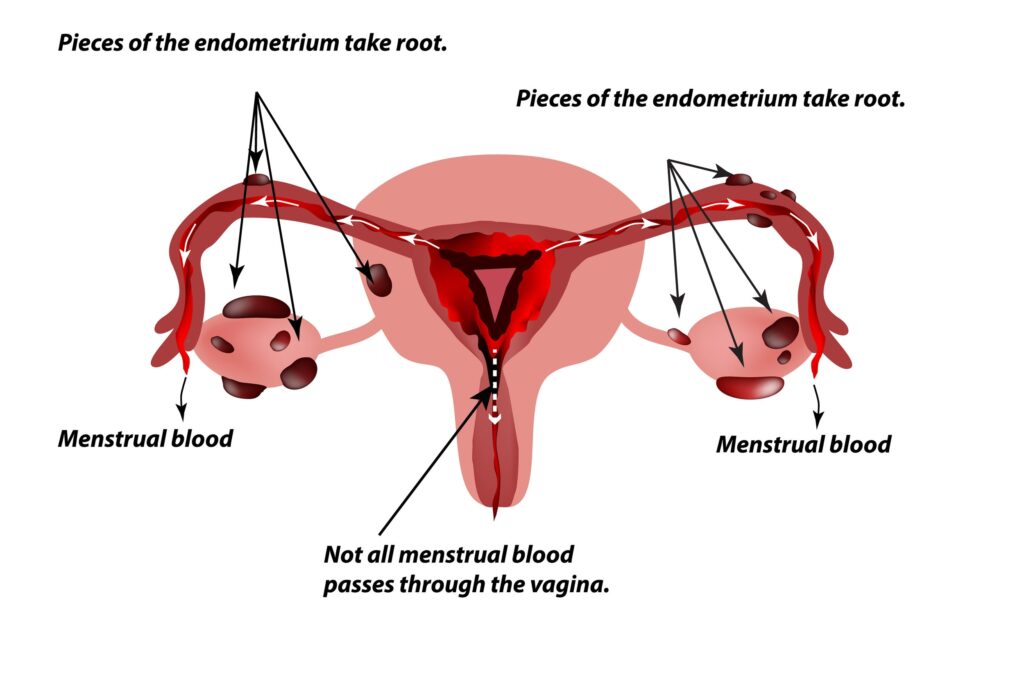
There’s also the theory of retrograde menstruation, where menstrual blood flows backward into the pelvis, allowing tissue to settle where it shouldn’t. Changes in the immune system may also make it harder for the body to clear this misplaced tissue.
Hormones, especially higher estrogen levels, can intensify symptoms, and environmental or inflammatory factors may influence how the disease progresses. Together, these factors help explain why endometriosis looks so different from one person to another.
How to Know If It’s Endometriosis or ‘Normal’ Period Pain
Normal period cramps are uncomfortable but usually:
- improve with simple pain medications
- last 1–3 days
- don’t disrupt your day-to-day life
With endometriosis, the pain is usually deeper, lasts longer, and affects your day-to-day life.
Early warning signs
These early symptoms often get ignored or normalised:
- cramps so severe you can’t walk, work, or attend school
- pain that worsens over time instead of improving
- heavy bleeding or bleeding between periods
- pelvic or lower back pain before, during, or after your period
- pain during or after sex (dyspareunia)
- fatigue that feels out of proportion to your activity
- bloating around your period (“endo belly”)
If your period pain regularly stops you from functioning, it’s not “just cramps.” Consider talking with a healthcare professional for a proper diagnosis.
Less obvious symptoms
Endometriosis can also affect the bowel, bladder, and in rare cases, areas like the diaphragm or chest.
You may notice:
- diarrhea
- constipation
- painful bowel movements
- stomach cramps that worsen during periods
- pain when urinating or needing to pee often
- blood in stool or urine during menstruation
- shoulder pain during your period (from diaphragm involvement)
- chest pain or trouble breathing around your period (rare)
These symptoms are often easy to treat one by one, like ‘just a stomach issue’ or ‘just an infection,’ without realizing they might be part of endometriosis.
Silent endometriosis
Some people have endometriosis with almost no cramps at all. Instead, they may struggle with:
- infertility
- ovarian cysts
- severe internal scarring
- incidental diagnosis during surgery for another issue
This is sometimes called silent endometriosis. The disease may still be progressing, but because the pain isn’t always extreme, it often gets missed or dismissed.
Why Endometriosis Is Often Missed in Africa
Across the continent, many women grow up believing that painful periods are “normal,” “a sign of strength,” or simply “what women are expected to handle.”
So many women end up pushing through the pain with over-the-counter pain medications, and silence, without realizing that this very endurance is what delays diagnosis.
Diagnosis is also harder because of several systemic and cultural barriers:
- Stigma around menstrual and sexual health: Many girls are taught not to talk about periods, pain, or “private parts,” so they hide symptoms until they become unbearable.
- Low awareness among the public and some healthcare professionals: Many women don’t know endometriosis exists, and some clinicians dismiss symptoms as “normal cramps” or “hormonal changes,” leading to repeated misdiagnosis.
- Limited access to gynecologists and laparoscopy in public hospitals: Most public facilities lack specialists and advanced imaging, meaning many women only get a diagnosis after years of untreated pain or infertility.
- Cultural expectations to endure pain quietly: In many homes, girls are praised for “being strong,” so even severe pain is normalized, and asking for help can be viewed as weakness or exaggeration.
Research shows that globally, a diagnosis can take 7–10 years, and this delay is often longer in African settings where symptoms are easily dismissed or misunderstood.
How Endometriosis Affects Daily Life
Endometriosis doesn’t just affect the body. Studies show it can influence how you work, study, relate to others, and feel about yourself.
For many African girls and women, this looks like:
- Missing school every month, getting labeled as “lazy” or “unserious” when you were actually too sick to go.
- Having trouble performing well at work due to flare ups, and being judged by others as untrustworthy or overly dramatic.
- Cooking, cleaning, or caring for family while in pain, often without rest and with no recognition of how heavy that burden is.
- Avoiding intimacy with your partner, due to the fact that sex hurts, and causing a lack of understanding from them.
- Living with chronic fatigue or physical exhaustion, for many years after being told “this is all in your head” or “you’re just making it up”.
Stages of Endometriosis
Doctors classify endometriosis into four stages based on how much tissue is present, how deep it grows, and whether cysts or scar tissue are involved.
Stage I: Minimal
A few small, shallow lesions with little to no scar tissue.
Stage II: Mild
More lesions than stage I, and they may grow a bit deeper into surrounding tissue.
Stage III: Moderate
Deep implants are present along with small ovarian cysts (endometriomas) and noticeable scar tissue.
Stage IV: Severe
Large cysts, extensive deep lesions, and dense adhesions that can cause organs to stick together.
However, the stage doesn’t always match how someone feels. A person with stage I may have disabling pain, while another with stage IV may have very mild symptoms.
How Endometriosis Is Diagnosed
There is no single blood test for endometriosis. Diagnosis usually involves:
- History and physical exam: A doctor will ask about your pain, periods, sex life, bowel habits, and family history. They may gently press your abdomen or do a pelvic exam to check for tender areas, swelling, or cysts.
- Pelvic ultrasound: A painless scan that uses sound waves to look at your uterus and ovaries. It can detect ovarian cysts but may miss small endometriosis lesions.
- MRI scan: A detailed imaging test that shows deeper lesions and organs clearly. It’s helpful for complex cases but expensive and not widely available in many regions.
- Laparoscopy: A minor surgical procedure where a small cut is made near the belly button and a camera is inserted to look directly at the organs. Doctors can confirm endometriosis and sometimes treat it during the same procedure.
In many African countries, laparoscopy is available mainly in private or referral hospitals, which makes early diagnosis harder for many women.
Treatment Options in Africa
Endometriosis has no permanent cure yet, but doctors can manage symptoms through medical care, lifestyle adjustments, and supportive strategies.
Pain relief and hormonal treatment
Common options include:
- NSAIDs such as ibuprofen or diclofenac
- combined birth control pills
- progestin-only methods (pills, injections, hormonal IUDs)
- GnRH agonists for severe cases
Surgical options
If medication isn’t enough, doctors may recommend laparoscopic surgery to remove or burn endometriosis lesions, release adhesions, and remove ovarian cysts.
Surgery can improve pain and fertility, but:
- symptoms can return
- costs may be high without insurance
- there is a shortage of trained endometriosis surgeons in many African regions
Supportive and lifestyle approaches
These don’t cure endometriosis, but they may help reduce flare-ups:
- gentle movement, like walking, stretching, or yoga
- stress-management practices, such as breathing exercises, meditation, or journaling
- anti-inflammatory diet, focusing on whole foods, fruits, vegetables, lean proteins, and omega-3 sources
- herbal remedies used with professional guidance, for example research shows that ginger may help ease menstrual pain
Always speak with a healthcare professional before combining herbs with hormonal medication to avoid potential interactions.
Frequently Asked Questions
Can endometriosis be cured?
There is no cure yet. Surgery and hormonal treatments can reduce or remove visible disease and relieve symptoms, but endometriosis can return.
How painful is endometriosis really?
Pain ranges from mild to completely disabling. It can feel like sharp stabbing, pulling, burning, or deep aching that doesn’t respond well to pain medications.
Is endometriosis common in African women?
Yes. Research suggests it is likely as common as in other regions, but many cases remain undiagnosed due to stigma, low awareness, and limited access to specialized care.
Conclusion
Endometriosis is a complex medical condition that affects your health, relationships, and your quality of life. For too long, severe menstrual pain has been dismissed as something women should simply endure, especially in African communities.
Recognizing symptoms early, seeking care, and understanding your treatment options can help you get the support you deserve. The more we talk about endometriosis, the more we reduce the silence and stigma surrounding it.
-

Muscular Dystrophy(MD): What it is Vs What you think it is
Muscular Dystrophy is one of those conditions that sits at the crossroads of genetics, family
health, and emotional reality. Across African communities, many parents and caregivers
encounter its signs without immediately recognizing them. Understanding what MD truly is
and what it is not can make a world of difference for early diagnosis and compassionate
support.
Muscular Dystrophy is essentially a genetic condition that affects the muscles, making
them weaker over time because they cannot produce the required proteins to keep them
strong. Think of muscles like a house; they need blocks (proteins) to stay firm. In MD, one or more of those “blocks” are missing or damaged. So over time, the “house” (the muscles) starts to break down.Muscular Dystrophy(MD) Is
- Not a tribe-based condition
- Not a punishment for anything your mother ate during pregnancy.
- Not contagious: You can hug, high-five, gist, and even eat from the same bowl with someone who has MD.
- Not laziness: A child struggling to climb stairs is not “forming slow motion” or serving attitude.
- Not caused by lack of exercise: You cannot exercise your way out of a genetic condition.
Muscular Dystrophy(MD) Is
- A genetic muscle disorder
- A progressive condition: Muscle weakness doesn’t happen overnight; it develops gradually and continues over time.
- A problem with muscle proteins: The body cannot make enough of the proteins needed to keep muscles healthy, so the muscle fibres slowly break down.
- A condition that affects daily movement: Walking, climbing stairs, lifting the arms, standing up, or even breathing may become more difficult as the muscles weaken.
- A lifelong medical condition: There is no cure yet, but treatments can improve comfort, mobility, and quality of life.
- A condition that can affect anyone: MD is not limited by tribe, region, gender, or lifestyle. It appears in all populations globally.
Types of MD
- Duchenne Muscular Dystrophy (DMD): Most common in children, mainly boys; causes rapid muscle weakness starting in the legs and pelvis.
- Becker Muscular Dystrophy (BMD: Similar to Duchenne but slower progression; symptoms appear later in childhood or adolescence.
- Myotonic Dystrophy: Causes prolonged muscle contractions (difficulty relaxing muscles) and can affect the heart and eyes.
- Limb-Girdle Muscular Dystrophy (LGMD): Affects muscles around the shoulders and hips.
- Facioscapulohumeral Muscular Dystrophy (FSHD): Weakens muscles of the face, shoulders, and upper arms; usually starts in teenage years.
- Congenital Muscular Dystrophy (CMD): Present at birth. It can cause delayed motor development and joint stiffness.
How can families and guardians identify MD?
The first step is simply being observant of the people in our closest space. How do they
move? What is their natural level of activity? Are they usually energetic, playful, or physically
confident? When a child or adult who was once active begins to slow down without a clear
reason, it can be an early signal that something is happening beneath the surface.
Muscular Dystrophy often reveals itself through gradual changes that families may notice
long before a formal diagnosis. These signs may include:- Frequent falls
- Trouble climbing stairs or keeping up with friends
- Tiring more quickly than other children or adults their age
- Struggling with tasks like lifting objects or running
For adults, early signs may be less obvious but still important, such as unusual muscle
fatigue, difficulty raising the arms, or gradual weakness in the hips and shoulders. Because MD progresses slowly, these symptoms may be mistaken for delayed growth, lack of fitness, or simply personality traits. As symptoms persist, it’s important to seek medical
attention as early detection facilitates better management.
Living with Muscular Dystrophy often means adapting to gradual changes in strength, stamina, and independence. Some people can walk and move freely for many years, while
others may need assistance earlier. These changes can affect daily activities like climbing
stairs, lifting objects or getting out of bed. Fatigue is also a common part of daily life. A short walk or basic activity may require more effort than usual, so pacing, rest, and support become important. Some individuals eventually rely on mobility aids such as braces, walkers, or wheelchairs, not as a sign of failure, but as tools that allow them to stay active and safe.Diagnosis: How Doctors Identify MD
A common first step is a blood test to check for high levels of muscle enzymes. When
muscles weaken or break down, these enzymes leak into the bloodstream and become
easier to detect. If the levels are unusually high, the doctor may investigate further.
From there, doctors may use genetic testing to check for specific gene changes linked to
MD. This is one of the most accurate ways to confirm the condition.Treatment and Management
Physical and occupational therapy help keep muscles strong, joints flexible, and daily
activities easier. Medications like steroids can slow muscle weakening, while other drugs
may protect the heart and lungs. Assistive devices such as braces, walkers, or wheelchairs
improve mobility and safety. In some cases, surgery may correct joint or spine problems.
Regular checkups are important to monitor the muscles, heart, and lungs, allowing early
treatment of complications.Living with Muscular Dystrophy comes with challenges, no doubt. With awareness,
medicine, and the support of family and friends, life can still be full of laughter and moments
of joy. Support makes a difference. Counselling, peer support groups, or simply talking with other families who understand can provide relief, comfort, and hope. Feeling seen, understood,
and supported can help both patients and caregivers navigate the emotional challenges of
MD. -
Epilepsy and Parkinson’s in Kenya
On a quiet morning in rural Kenya, a young girl suddenly falls to the ground, her body convulsing. Her mother rushes her inside as neighbors gather. She has just had a seizure in public. Whispers of witchcraft spread quickly. Fearing judgment, the family keeps her hidden at home rather than taking her back to school.
This is the reality for many families in Kenya living with neurological conditions like epilepsy and Parkinson’s. Across the country, these conditions remain widely misunderstood and stigmatized. Instead of being recognized as medical conditions, they are often linked to curses or punishment, turning treatable conditions into sources of shame and isolation.
What is Epilepsy
In Kenya, about 1 in every 100 people lives with epilepsy. Research from 2022 shows that rates in rural coastal areas can be up to six times higher than the global average.
Epilepsy is a brain disorder that causes sudden bursts of abnormal electrical activity, disrupting normal brain function and triggering seizures.
These seizures can vary depending on the type and part of the brain involved. Some may be subtle, such as brief staring episodes, while others trigger full body convulsions.
Common symptoms include:
- sudden jerking or shaking of the body
- brief loss of awareness or staring spells
- confusion or memory lapses after an episode
- unusual sensations like strange smells or tingling before a seizure
- repeated seizures, which can differ from person to person
The Centers for Disease Control and Prevention (CDC) notes two main types of seizures:
- Focal seizures: These start in one area of the brain and may happen with or without loss of awareness.
- Generalized seizures: These affect both sides of the brain and often cause loss of consciousness.
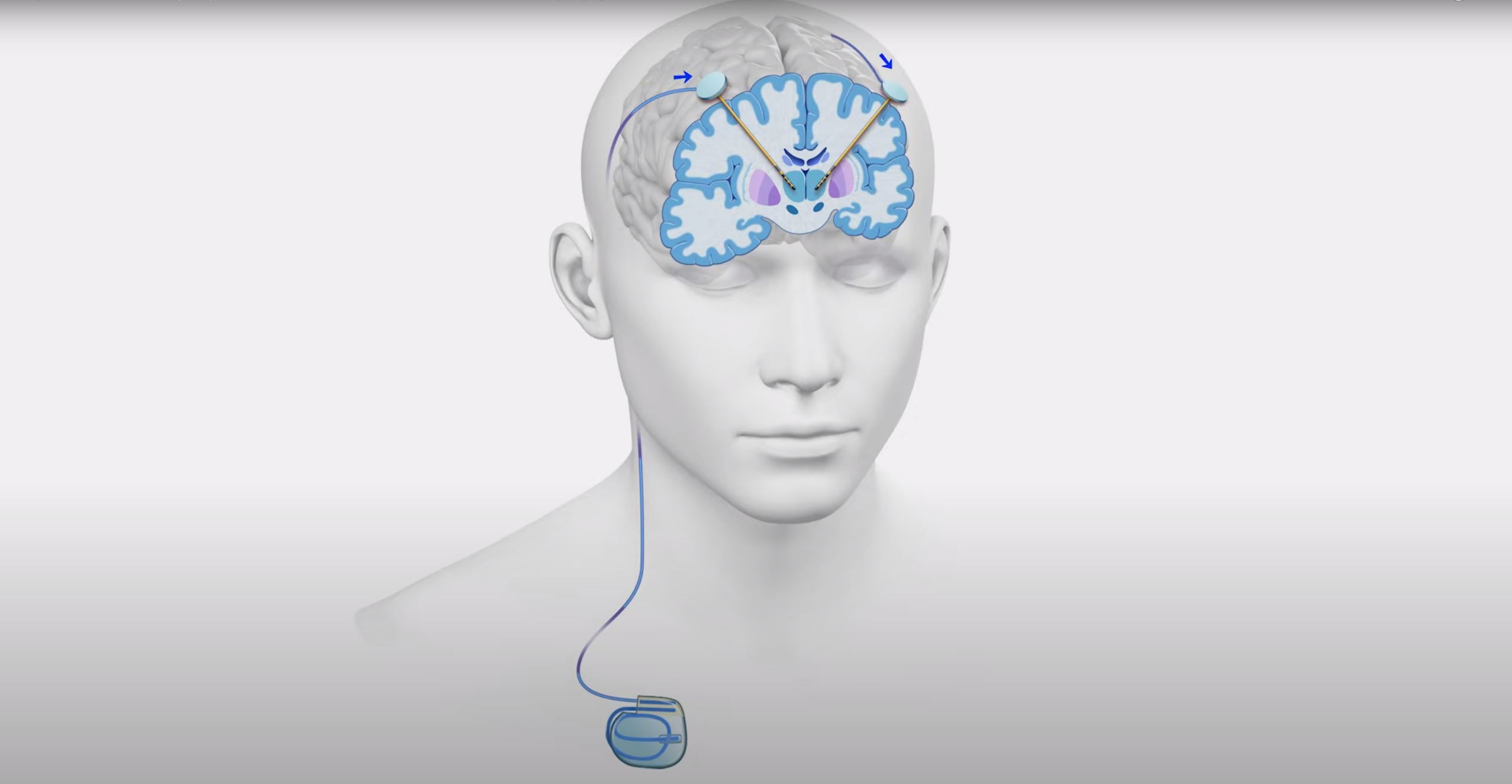
What is Parkinson’s?
Parkinson’s disease is a chronic condition that affects how the body moves. It occurs when the brain slowly loses dopamine, the chemical messenger that helps muscles work smoothly.
Typical symptoms of Parkinson’s include:
- slowed movement
- muscle stiffness or rigidity
- tremors (shaking, often in the hands or fingers)
- changes in balance and posture
- reduced facial expression or softer speech
While there’s currently no cure for either epilepsy or Parkinson’s, treatments and therapies can relieve symptoms and improve quality of life.
Are epilepsy and Parkinson’s a curse or a condition?
Epilepsy and Parkinson’s are medical conditions, not curses. They are not contagious and have no link to witchcraft, spirits, or punishment. Yet in many Kenyan communities, seizures are still seen as signs of evil spirits, witchcraft, or ancestral punishment. Families may first turn to traditional healers instead of hospitals.
Some even believe that touching someone during a seizure could “transfer” the condition, a myth that keeps families silent and afraid. Parkinson’s, which causes tremors and changes in movement, is sometimes mistaken for possession, alcoholism, or “old age gone wrong.”
These beliefs create fear and shame, leading families to hide loved ones or delay medical care, which only worsens outcomes.
How does stigma affect people living with these conditions?
The stigma attached to epilepsy and Parkinson’s often hurts more than the condition itself:
- Children and education: A child with epilepsy may be expelled after a seizure in class. Teachers fear disruption, and parents of other children fear “catching it.”
- Marriage and family life: Women with epilepsy are sometimes labeled “unfit for marriage.” and spouses may also abandon partners diagnosed with Parkinson’s.
- Employment: People are denied jobs because employers assume they are unsafe or unreliable.
- Social belonging: Many families hide their relatives with seizures or tremors to avoid gossip. Weddings, funerals, even church services become out of reach.
This stigma doesn’t just affect health, it also creates deep loneliness and shame. In some cases, families even abandon their loved ones in hospitals because of it.
Why is access to care still so hard in Kenya?
Access to care for epilepsy and Parkinson’s in Kenya is still hard, because even when families overcome stigma, they encounter health system barriers such as:
- Too few specialists: Kenya has fewer than 30 neurologists for more than 55 million people, most based in Nairobi.
- High costs: Anti-seizure and Parkinson’s drugs are expensive without insurance. Many families ration doses or stop treatment.
- Rural divide: County hospitals often lack diagnostic tools and trained staff. Travel costs make treatment difficult for many.
- Policy gaps: Neurological conditions are often left out of national health plans, which focus more on infectious diseases.
How can we break the cycle of stigma?
Breaking the stigma is possible, and it’s already happening. Here’s how:
- Awareness campaigns by NGOs and advocacy groups are teaching communities that seizures are not curses, and tremors are not “old people problems.”
- Inclusive schools that train teachers to support children with epilepsy, rather than expelling them, can change an entire community’s perception.
- Families that seek medical care set an example. A child returning to school after treatment, or an older man walking again with therapy, can shift how an entire community thinks.
- Faith leaders and the media are important allies in shifting cultural narratives. Churches, mosques, and radio stations are helping spread facts instead of fear.
Breaking stigma is not just about medications. It’s about compassion, education, and refusing to let myths define people’s lives.
Frequently Asked Questions (FAQ)
Here are some frequently asked questions about epilepsy and Parkinson’s disease.
What is the main cause of epilepsy?
There isn’t one main cause of epilepsy. It may result from brain injury, infections, stroke, or genetics.
Can you live a normal life with Parkinson’s?
Yes. People with Parkinson’s can live a fairly normal life in the early stages when symptoms are mild, but as the disease progresses, they need more treatment and support in daily life.
What is the first aid for a seizure?
Stay calm, move objects away, and place the person on their side so they can breathe. Do not put anything in their mouth. If the seizure lasts longer than 5 minutes, seek medical help.
Conclusion
In Kenya, epilepsy and Parkinson’s carry a heavy stigma. Families stay silent, children are kept from school, and many people miss out on the care they need. But these are not curses. With treatment, people can manage these conditions, and they deserve to live with dignity and understanding.
-

When Hives Don’t Go Away: Chronic Urticaria
Most people have had hives at least once, those itchy, red, swollen patches that appear suddenly and usually fade within a few hours or days. But when hives last for more than six weeks, they fall into a category called chronic urticaria. This condition can be frustrating, unpredictable, and sometimes misunderstood.
What is Chronic Urticaria?
Chronic urticaria (CU) is a long-lasting form of hives where red, itchy welts or swelling appear on the skin almost daily or frequently for six weeks or more. Unlike short-term hives, which often have an obvious trigger (like a food allergy or insect bite), chronic urticaria is harder to pin down and can linger for months, or even years.
What Are The Symptoms?
- Raised, red, or skin-colored welts (hives) that may change shape and location
- Intense itching, sometimes worse at night
- Swelling of the lips, eyelids, hands, or feet (angioedema)
- Flare-ups that come and go, even without a clear trigger
What Causes It?
In many cases, chronic urticaria has no clear cause. Doctors call this chronic spontaneous urticaria. But sometimes, underlying issues may play a role:
- Immune system activity: The body mistakenly releases histamine, a chemical that triggers itching and swelling.
- Infections: Some chronic infections (such as Helicobacter pylori in the stomach) may contribute.
- Other health conditions: Thyroid disease, autoimmune disorders, or hormonal shifts can sometimes be linked.
- Physical triggers: Heat, cold, pressure on the skin, exercise, or stress may worsen symptoms.
Diagnosing Chronic Urticaria
There isn’t a single test that confirms chronic urticaria. Diagnosis usually involves:
- A physical exam and review of symptoms
- Blood tests to rule out thyroid or autoimmune issues
- Allergy testing (sometimes)
- Keeping a symptom diary to track triggers
Living With Chronic Urticaria
The daily experience can be exhausting, with the constant itchiness, unpredictable flares, and worry about appearance, which may affect sleep, work, or social life. Beyond physical symptoms, many people also deal with anxiety or frustration because the condition can feel invisible to others.
Managing the Condition
While there’s no universal cure, several strategies can help:
- Avoid known triggers: If stress, certain foods, or temperature changes seem to set off hives, reducing exposure may help.
- Skin care: Use gentle, fragrance-free soaps and moisturizers. Cool compresses can soothe itching.
- Lifestyle: Wearing loose clothing, avoiding overheating, and managing stress may reduce flare-ups.
- Medical care: Doctors often recommend antihistamines to control symptoms, but treatment should be tailored to each person.
The Takeaway
Chronic urticaria is more than just a skin condition, it affects quality of life. While it can be long-lasting, it is manageable with the right support and care. If you notice hives that don’t go away after several weeks, or if swelling affects your lips or breathing, the safest step is to see a doctor. They can rule out serious causes and help you find the right management plan.
Frequently Asked Questions
1. What is chronic urticaria?
Chronic urticaria is a condition where itchy hives or swelling keep appearing almost daily or frequently for six weeks or longer.2. What causes it?
In many cases, the exact cause is unknown (this is called chronic spontaneous urticaria). Sometimes, it may be linked to autoimmune reactions, thyroid disease, stress, infections, or physical triggers like heat, cold, or pressure on the skin.3. Is chronic urticaria an allergy?
Not always. While allergies can cause hives, most cases of chronic urticaria are not allergic reactions. Instead, they happen when the immune system mistakenly releases histamine and other chemicals.4. Can stress make it worse?
Yes. Stress doesn’t directly cause urticaria, but it can trigger flare-ups or make existing hives more intense.5. How is chronic urticaria treated?
The main treatment is non-drowsy antihistamines. In more severe cases, doctors may recommend stronger medications like corticosteroids (short-term), omalizumab (an injection), or immunosuppressants.6. Can it be cured?
There is no permanent “cure,” but most people find that the condition improves or goes away over time. Management focuses on controlling symptoms and identifying possible triggers.7. Should I see a doctor?
Yes. If hives last longer than six weeks, or if they are accompanied by swelling in the lips, tongue, or throat (angioedema), you should seek medical attention immediately. - Raised, red, or skin-colored welts (hives) that may change shape and location
-
Your Child Is Not an Olodo — They May Have Dyslexia
Globally, dyslexia affects about 1 in 10 people, but awareness remains low across Africa. In classrooms across West Africa, children who struggle to read are often reduced to cruel names. A Nigerian child might be called “olodo.” In Ghana, “blockhead.” In francophone countries like Mali or Guinea, “bête.”
What Dyslexia Really Is
Dyslexia is a specific learning disorder that affects how the brain processes written and spoken language. Children with dyslexia have trouble reading, spelling, and sometimes writing, even though they may have normal or above-average intelligence. It is not caused by laziness, it’s a neurological difference in how the brain interprets symbols and sounds.
What Causes Dyslexia?
The exact cause isn’t fully understood, but research shows that dyslexia often runs in families and is linked to how the brain’s language areas develop. Factors include:
- Genetics: Children with a parent or sibling who has dyslexia are more likely to have it.
- Brain structure and function: Brain imaging shows that people with dyslexia use different pathways when processing language.
- Premature birth or low birth weight: These may increase the risk.
- Early language difficulties: Trouble recognizing sounds in words can signal later reading challenges.
Dyslexia is not caused by poor parenting, laziness, or lack of intelligence.
Signs of Dyslexia in Children
Dyslexia can show up differently depending on age:
Preschool years:
- Trouble learning nursery rhymes
- Difficulty recognizing letters or rhyming words
Primary school years:
- Mixing up letters (like “b” and “d”, p and q)
- Reading slowly or skipping words while reading
- Struggling to spell common words
- Avoiding reading out loud in class
Teen years and beyond:
- Reading far below grade level
- Difficulty summarizing a story
- Trouble learning new languages
- Strong verbal or creative skills, but continued struggle with written tasks
Diagnosing Dyslexia
Diagnosis usually involves:
- Educational assessments: Tests for reading, writing, memory, and language skills.
- Family history review: Looking for learning difficulties among relatives.
- Professional evaluation: Carried out by psychologists, special educators, or speech-language therapists.
Early diagnosis is importantl. The earlier dyslexia is identified, the easier it is to support learning and build confidence.
Supporting a Child With Dyslexia
There is no “cure” for dyslexia, but children can thrive with the right strategies:
Educational support
- Phonics-based reading programs that teach sound–letter connections
- Multi-sensory teaching (using sight, sound, touch, and movement to reinforce learning)
- Extra time in exams or assignments
Home support
- Read with the child daily in a calm, patient way
- Celebrate strengths in creativity, art, or problem-solving
- Encourage, rather than punish, when mistakes happen
Professional help
- Speech-language therapy to improve reading and writing
- Special education programs tailored to learning differences
Myths About Dyslexia
- Myth: Dyslexia means a child is unintelligent.
Fact: Dyslexia is unrelated to intelligence; many people with dyslexia are highly creative and successful. - Myth: Dyslexia can be “outgrown.”
Fact: It doesn’t go away, but children can learn strategies to read and write more effectively. - Myth: Children with dyslexia just need to try harder.
Fact: They are already trying hard; they just need different learning methods.
Frequently Asked Questions (FAQ) About Dyslexia
Can dyslexia affect any child?
Yes. Dyslexia can affect children of any culture, background, or intelligence level.Is dyslexia the same as bad handwriting?
No. Dyslexia is specifically about difficulties with reading and spelling, though some children may also struggle with handwriting.Does dyslexia mean a child will fail in life?
Not at all. With proper support, children with dyslexia can excel in school, careers, and life. Many successful leaders, entrepreneurs, and artists have dyslexia.Should I see a professional if I suspect my child has dyslexia?
Yes. Early evaluation by an educational psychologist or speech-language therapist helps identify dyslexia and start the right support. - Genetics: Children with a parent or sibling who has dyslexia are more likely to have it.
-

Hirsutism Is Not An ‘Igbo Women’s Problem’
In Nigeria, hirsutism is sometimes unfairly framed as an “Igbo women’s problem,” a stereotype that distracts from the real medical causes. Online forums often fuel these myths, linking excess hair growth to ethnicity or “good genes.” But in reality, hirsutism is a medical condition with biological explanations, not cultural ones.
What Hirsutism Really Is
Hirsutism (pronounced HUR-soot-iz-um) is a medical condition in women that causes excessive growth of coarse, dark hair in areas where men typically grow hair such as the chin, chest, stomach, or back.

What Causes Hirsutism?
Hirsutism happens when the body produces too much of the male hormone called androgens. Women naturally produce androgens, but usually in small amounts. When levels rise above normal, it can trigger excess hair growth as well as other changes, such as acne, voice deepening, or differences in body shape.
In some cases, hormone levels look normal, but the hair follicles are extra sensitive to androgens. This sensitivity alone can cause thick, dark hair to grow in areas where women typically do not have it.
Some common reasons for higher androgen activity include:
Polycystic Ovary Syndrome (PCOS): A hormonal condition that often leads to small cysts on the ovaries and disrupts the balance of estrogen and androgens.
Cushing’s Syndrome: Caused by long-term exposure to high levels of cortisol, the body’s main stress hormone.
Hormone-producing tumors: Rare growths in the ovaries or adrenal glands that increase androgen production.
Certain medications: Drugs like anabolic steroids, treatments that encourage hair growth (such as minoxidil), or danazol (used for endometriosis) can lead to unwanted facial or body hair.
High insulin levels: When insulin is too high, it can push the ovaries to release more androgens.
Congenital adrenal hyperplasia: An inherited condition that affects how the adrenal glands make hormones, sometimes leading to excess androgen.
Menopause: Hormonal shifts after menopause may cause new or increased facial and body hair.
Idiopathic causes: Sometimes, no medical explanation is found.
PCOS VS Hirsutism
Polycystic Ovary Syndrome (PCOS) is one of the most common causes of hirsutism, but they are not the same condition. Women with PCOS often have additional symptoms like irregular periods, acne, weight changes, or fertility struggles. Hirsutism, on its own, may appear without any other PCOS signs.
Diagnosing Hirsutism
Doctors usually begin with a physical exam, checking hair growth patterns and related symptoms. To understand the root cause, they may recommend:
- Blood work to measure hormone levels.
- Ultrasound scans to check the ovaries and uterus for cysts or irregularities.
- CT scans or X-rays of the adrenal glands to rule out abnormalities.
- MRI scans if a problem in the brain or pituitary gland is suspected.
- Pelvic examination to look for ovarian cysts or tumors.
They may also use the Ferriman–Gallwey scale, which scores hair growth across nine body areas from 0 to 4. A higher total score signals more severe hirsutism.
Treating Hirsutism
Treatment depends on the cause, severity, and personal preference. Options include:
Lifestyle and self-care
- Weight management: Losing weight can lower androgen levels.
- Shaving, tweezing, waxing, or threading: Common but temporary methods of hair removal.
- Depilatory creams: Break down hair chemically (patch test recommended).
- Bleaching: Lightens hair to make it less visible.
Medical and long-term options
- Laser hair removal: Uses heat to damage follicles; may require multiple sessions.
- Electrolysis: Permanently destroys hair follicles using electric current.
- Medications:
In some cases, doctors may prescribe medications to help manage symptoms or address hormone imbalances. The specific choice depends on the individual’s diagnosis, and only a healthcare provider can determine what’s safe and effective.
Hair growth patterns are complex, medical, and individual. They are not tied to tribe, culture, or stereotypes. If you notice unusual or distressing hair growth, the best step is to see a qualified doctor who can identify the underlying cause and guide you toward safe, effective care.
Frequently Asked Questions (FAQ) About Hirsutism
Is hirsutism the same as just being hairy?
No. Many women naturally have body hair. Hirsutism refers specifically to coarse, dark hair growing in areas where women don’t usually grow much hair, like the chin, chest, or back.Can hirsutism affect any woman?
Yes. Hirsutism can affect women of any tribe, race, or background. It’s not linked to ethnicity or culture—it’s a medical condition.Is hirsutism always caused by PCOS?
Not always. PCOS is a common cause, but hirsutism can also be linked to hormonal imbalances, certain medications, menopause, or even run in families without an obvious medical cause.Can hirsutism go away on its own?
Sometimes mild cases improve with lifestyle changes, like weight management. But often, a medical evaluation is needed to find and treat the root cause.Does hirsutism mean I can’t get pregnant?
Not necessarily. While conditions like PCOS can affect fertility, hirsutism itself does not automatically mean infertility. Many women with hirsutism conceive and have healthy pregnancies.Should I see a doctor about hirsutism?
Yes, especially if the hair growth is sudden, severe, or accompanied by other symptoms like irregular periods, acne, or voice changes. A doctor can check for underlying health conditions and recommend safe treatment options.